
The “Count” is a required Standard of Practice in any OR regardless of acuity, volume, urgency, or anything else for that matter. This principle is mandatory to meeting Quality Assurance and is put in place for the Standard of Care to be met.
With the rising demands of Healthcare and the associated need for Nurses, many clinical practices have lacked reinforcing the Standard of Care. Consequently, negatively impacting the culture of the OR and facility. The Count is detrimentally one of them.
A Cesarean Section was about to proceed and documented as semi-urgent on a busy Labor and Delivery Unit. Meaning, the Labor was no longer progressing, and medical management of that Labor was no longer effective. The “Section” was slated for a workable time for the Unit and staffing, indicating the sense of urgency it held for Mom and Baby. The Section rate in this Department was 60%. That’s correct – 60% – an astronomically higher than average rate nationally. Therefore, they had plenty of practice and ample opportunity to get it right.
The Section proceeded unremarkably, and the Surgeon was closing with the accompaniment of an experienced Scrub Tech. Anyone who has worked in an OR can grasp its normalcy being a workplace setting like any other where staff socializes while simultaneously suturing a patient. The Circulator for the case thought an extraordinary amount of time was passing for the first cavity count to begin. Upon looking at the Field, this Circulator realized the Intra-Operative period was 2″ from closing skin. The Surgeon and Tech were questioned, ignored the repeated requests to stop for Count, and continued to close.
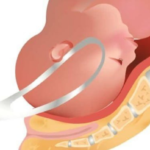
The Surgeon promptly left the room within a minute of End Time and returned to the clinic. Following an exasperating search of 30 minutes for a missing sponge, a portable x-ray was called. With the patient still on the table, the sponge was quickly located. The Surgeon informed and consequently easily retrieved before fascia. A Sentinel event had now occurred, generating the appropriate documentation and departments notified, including Risk Management.
Several days later, a debriefing was called, and the case was reviewed. The written protocol of the Count was used to determine fault and the Circulator for this case held 100% accountable. Why? Because they are responsible for 95% of the tasks in the OR. However, more variables were involved than the Circulator not identifying 2 of the 4 Counts being missed, one being late, and the Surgeon leaving before hearing the infamous words “final count correct”.
For the past two years upon the Circulators hiring to the Unit, it was brought to Administration’s attention and all staff, including Surgeons, what a “sloppy” count the Unit had and the need to change this practice. This was documented, including several meetings held to rectify this and consequently meet Standards. Some improvements were made, but consistency continued to lack the Standard rarely ever met.
Who was responsible for the sponge left inside the patient? The Circulator? Tech? Surgeon Department?
Where did that Department fail when they dismissed the Nurse’s concerns of the “Count”?